We’re talking about babies the size of kittens here, whose respiratory systems and major organs are completely underdeveloped. It’s not maybe changing nappies. It is a high pressure, highly skilled job. It’s one on one, constant monitoring, checking their temp and vitals, checking their gases, checking their lines, checking their tubes, checking their ventilation, feeding them, giving them fluids, administering their medication, cleaning them, supporting the family, documenting everything, and yes obviously changing their nappy. That’s constant monitoring, constant hands in incubator. These nurses are replacing a human placenta.
Even for the babies who required that one on one care, most of time at COCH they didn’t get it. Often nurses would have more than one baby in nursery 1, or worse: babies spread across different rooms. Since every medication requires two nurses, they were also often pulled away from their babies to assist others, or to cover for everyone else’s break time, when really they should only be leaving their own babies to assist with emergencies.
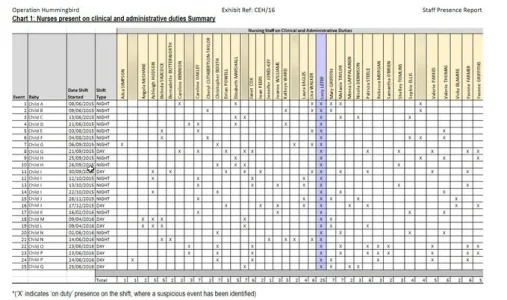
While this kind of staffing might be “normal” in modern day NHS, it is nowhere close to optimal. If a baby is supposed to be receiving 100% of a nurse’s time, it might end up with only 25% depending on the circumstances of the shift. COCH had too many babies, too many one on one babies, and too few staff. There are days on that chart where there were only 4 nurses on shift, each of which will require a break, and we know the unit was housing up to 20 babies at a time (which might be fine if they’re all room 4 babies, but we know that wasn’t the case). When you’re operating a skeleton staff like that, alongside out-of-their-depth doctors who were intimidated by the NNU and preferred to be in the paediatric ward, then when things go downhill, they go downhill fast.
So yes, no space for oversight. But these nurses are absolutely run ragged, juggling and reprioritising constantly, not just hanging around to do the odd feed or nappy.